
DSM-5 Criteria for PTSD
All of the criteria are required for the diagnosis of PTSD. The following text summarizes the diagnostic criteria:
Criterion A: stressor (one required)
The person was exposed to: death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence, in the following way(s):
- Direct exposure
- Witnessing the trauma
- Learning that a relative or close friend was exposed to a trauma
- Indirect exposure to aversive details of the trauma, usually in the course of professional duties (e.g., first responders, medics)
Criterion B: intrusion symptoms (one required)
The traumatic event is persistently re-experienced in the following way(s):
- Unwanted upsetting memories
- Nightmares
- Flashbacks
- Emotional distress after exposure to traumatic reminders
- Physical reactivity after exposure to traumatic reminders
Criterion C: avoidance (one required)
Avoidance of trauma-related stimuli after the trauma, in the following way(s):
- Trauma-related thoughts or feelings
- Trauma-related external reminders
Criterion D: negative alterations in cognitions and mood (two required)
Negative thoughts or feelings that began or worsened after the trauma, in the following way(s):
- Inability to recall key features of the trauma
- Overly negative thoughts and assumptions about oneself or the world
- Exaggerated blame of self or others for causing the trauma
- Negative affect
- Decreased interest in activities
- Feeling isolated
- Difficulty experiencing positive affect
Criterion E: alterations in arousal and reactivity
Trauma-related arousal and reactivity that began or worsened after the trauma, in the following way(s):
- Irritability or aggression
- Risky or destructive behavior
- Hypervigilance
- Heightened startle reaction
- Difficulty concentrating
- Difficulty sleeping
Criterion F: duration (required)
Symptoms last for more than 1 month.
Criterion G: functional significance (required)
Symptoms create distress or functional impairment (e.g., social, occupational).
Criterion H: exclusion (required)
Symptoms are not due to medication, substance use, or other illness.
Two specifications:
- Dissociative Specification In addition to meeting criteria for diagnosis, an individual experiences high levels of either of the following in reaction to trauma-related stimuli:
- Depersonalization. Experience of being an outside observer of or detached from oneself (e.g., feeling as if "this is not happening to me" or one were in a dream).
- Derealization. Experience of unreality, distance, or distortion (e.g., "things are not real").
- Delayed Specification. Full diagnostic criteria are not met until at least six months after the trauma(s), although onset of symptoms may occur immediately.
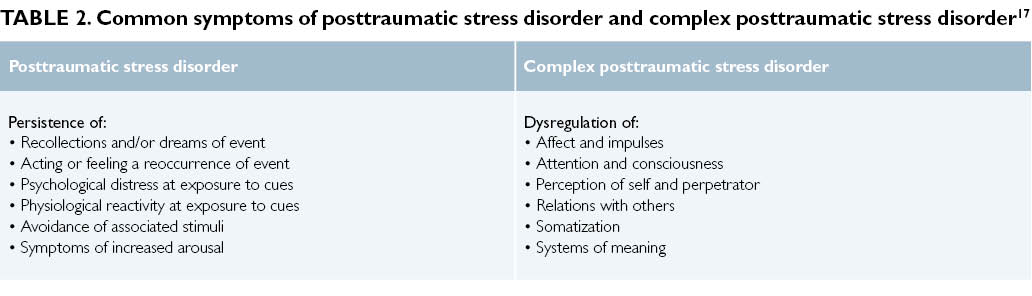
Complex PTSD (C-PTSD)
When the Trauma Doesn't End
First proposed by Judith Herman in her 1992 book, Trauma and Recovery, she suggested people dealing with child physical abuse, intimate partner violence, women trapped in sexual slavery, and other people experiencing long-term stress often showed symptoms very different from people experiencing single-event traumas. As a result, they can often become passive and withdrawn (due to learned helplessness), or develop highly unstable personalities. This could lead to dangerous repetitive behaviours such as becoming involved with violent partners, repeated self-harm attempts, or chronic substance abuse.
Though not part of the new DSM-5, suggested C-PTSD symptoms in adults include:
- Difficulties regulating emotions, including symptoms such as persistent sadness, suicidal thoughts, explosive anger, or covert anger
- Variations in consciousness, such as forgetting traumatic events (i.e., psychogenic amnesia), reliving traumatic events, or having episodes of dissociation (during which one feels detached from one's mental processes or body).
- Changes in self-perception, such as a chronic and pervasive sense of helplessness, shame, guilt, stigma, and a sense of being completely different from other human beings.
- Varied changes in the perception of the perpetrator, such as attributing total power to the perpetrator or becoming preoccupied with the relationship to the perpetrator, including a preoccupation with revenge.
- Alterations in relations with others, including isolation, distrust, or a repeated search for a rescuer.
- Loss of, or changes in, one's system of meanings, which may include a loss of sustaining faith or a sense of hopelessness and despair.
- behavioural problems,
- poor impulse control,
- pathological self-soothing (through dysfunctional coping mechanism such as self-cutting), and
- sleep problems.
Developmental Trauma Disorder (DTD)
Since C-PTSD does not adequately reflect the kind of developmental impact seen in children, clinicians have suggested an alternative diagnosis, Developmental Trauma Disorder (DTD).
DTD, also paralleled with complex PTSD (CPTSD), is caused by chronic and multifaceted traumatic events that occur during childhood that permanently influence a developing brain, affecting emotional and cognitive function and behavior.
Traumatized children meet the DSM diagnostic criteria for many disorders, such as PTSD, but the various symptoms of DTD or CPTSD are not completely listed in the PTSD criteria and are often labeled as comorbidities.
Most recently, DSM modifications for PTSD included a subtype group for children aged younger than 6 years. Research has shown when diagnostic criteria that are sensitive to child developmental stages were used, together with an appropriate behavioral assessment, more children qualified for a diagnosis of the child PTSD subtype than any other PTSD groups.
Child PTSD evaluation include a lack of verbal skills in reporting abuse and the manner in which trauma-related symptoms and memory are expressed. For example, decreased interest in routine activities and play or “restricted play” are considered, and severe temper tantrums are noted to represent increased arousal behavior.
Other childhood signs of PTSD include “loss of interests, restricted range of affect, detachment from loved ones, and avoidance of thoughts or feelings related to the trauma.” These symptoms are typical for children but are less distinct in adults with PTSD.
In short, victims of childhood trauma exhibit many symptoms of PTSD, including dissociation, guilt, and hopelessness, but the diagnostic criteria for PTSD does not accurately include all the important indicators of DTD. Developmental Trauma Disorder: the effects of child abuse and neglect by Maureen V. Kilrain, MS, PA-C
Edited to add: Something we often forget is that we, the parents, can experience PTSD or Secondary PTSD. Working with children with trauma and/or attachment issues can be a very traumatizing experience. It can also trigger issues from our own past that we may have thought we had dealt with long ago. Please get help for yourself and take care of you! Parents get overwhelmed too. If we ignore ourselves and give until there is nothing left then we can no longer function as parents or even just as people.
Some resources: http://www.psychologytools.org/ptsd.html
What Worked for Us
My children have many overlapping diagnoses, and what works for one doesn't always work for the other, but here are some of the things we've found to help when adopting an older child with known Complex PTSD (C-PTSD):
Therapists
Get a good therapist who understands and has experience working with adopted/foster kids with trauma. We love our EMDR therapist for our daughter but still use a good attachment therapist too.
NOTE: Don't be afraid to "fire" the therapist if it's not a good personality match.
EMDR Therapy
EMDR is the most recommended therapy for people with PTSD. It is most often used by soldiers and victims of trauma (like rape or being in a natural disaster), and usually only requires 2-3 sessions.
Obviously, people who have suffered from long-term trauma (Complex PTSD), such as child abuse, would most likely require more sessions.
Medications
There are no meds specifically for treating PTSD, but with good therapy and meds that help with the symptoms, the child can recognize the effects of the trauma, learn to cope, and move on to dealing with the cause of the trauma.
Overlapping Diagnoses
Don't be surprised if PTSD is not your child's only diagnosis, adopting older children usually means they have more going on then just one issue - attachment disorders, physical and sexual abuse, bipolar disorder, ADHD, FAS/FAE...
Caseworkers will not or cannot tell you all of what caused the PTSD, and often symptoms overlap and appear to be other things. I don't think I've ever heard of a child with RAD that didn't also have PTSD. Here's a good chart for Overlapping Behavior Characteristics.
TRIGGERS
- Puberty
Puberty will exacerbate the problem. Be sure you do everything you can to facilitate attachment before it hits and be ready for some regression. {The Teen Years} - Bedtime
Bedtime can be a huge PTSD trigger, often causing Night Terrors and nightmares. Our son frequently has trouble going to sleep, sleeping through the night, and during a particularly bad period, would wake up with his heart pounding and his body shaking all over (his central nervous system releasing stored memories). His "nightmares" of the devil were so real he thought they were visions. Hubby and I took turns sleeping near him for a week. {Sleep Issues} - Projecting on Others (especially parents)Be prepared for your child to blame you for their past. My daughter recently admitted to seeing one of her past abuser's face everywhere - on walls, and particularly - over my husband's face. She hates "him," rages at him, tells him he is mean and evil, accuses him of yelling at her (even though Hubby isn't even raising his voice) and dissociates.
- Stimulating/ Overwhelming Situations
We avoid big groups, noisy places, and in particular, any situation that we know could trigger a flashback. I strongly recommend this, particularly for the first 6 months the child is in your home. Especially avoid the temptation to travel, have a party, introduce your child to everyone, shower him with gifts - he's already dealing with an overwhelming number of changes just by moving into a new home with a new family. - Stimulating Environments
Avoid stimulating events, situations, etc. We have our daughter and son's rooms stripped down to the bare essentials, not just because they've done lots of damage, but because anything more is overwhelming.
Fight/ Flight/ Freeze
When in a meltdown Kitty mentally shuts down - we call it fight, flight, or freeze. She is acting instinctually to protect herself. The thinking part of her brain is not "online."
It's difficult not to hold her accountable when she rages during these times, but we've learned to wait until she's calm and then process what led up to the event so we can help her prevent re-occurrences. There are times when she doesn't remember the meltdown/ rage happening at all. {Handling Rages}
School
Some suggestions for dealing with schools. PTSD is rarely recognized in schools. My children have behavior issues as well as diagnoses that require an IEP (including OHIs -other health impairment- like ADHD). Once you get an IEP though, you can access behavior accommodations that can really help.
Look for knowledgeable parent liaisons who will help you find the resources and accommodations your child needs. Be aware that no matter how wonderful and helpful the school seems, they usually will not volunteer information, and they may actually discourage you from getting help.
Request an assessment of your child in writing - they have 30 days to respond. Make sure they know you are willing to get or have gotten, in touch with an advocate/ lawyer.
ADVOCATE for your child. NO ONE else is as qualified as you are about your child's needs.
My Top 10ish Things I Couldn't Do This Without
I've written a lot of posts on things like Why Won't My Child Just Behave? and Why Doesn't My Child Feel Safe? maybe one of them will have some ideas for you.
Read Beyond Consequences, Logic and Control. It really helped us understand why our kids act the way they do sometimes (they are SCARED!). I also liked Parenting with Love and Logic - it's for "neurotypical" kids so a lot of it doesn't apply to kids of trauma, but it helped me stay calm!
Prioritizing Yourself, Your Family, and Your Child - In That Order!
Get lots of support and take good care of yourself, your husband and your marriage.
Self-Care
Try to surround yourself with people who "get it." In person is best, but the internet has lots of great parent support groups, including BeTA http://www.momsfindhealing.com/ and Facebook groups like the one I admin - Parenting Attachment-Challenged Children and others like Parenting with Connection.
We as parents often get our own PTSD, CTS (Continuous Traumatic Stress), and Caregiver Fatigue. Please take care of yourself!!
__________________
Kitty - came into our home at 11, now 13 - originally diagnosed with ADHD, ODD, learning disabilities, attachment "issues" and victim of abuse. Now diagnosed with bipolar, attachment disorder, ODD, Complex PTSD, learning disabilities, and victim of abuse.
Bear - Kitty's 1/2 sibling, came into our home at 13, now 15 - originally diagnosed with PTSD, conduct disorder, victim of abuse and mood disorder. Now diagnosed with bipolar, RAD, ADD, PTSD, cerebral dysrhythmia, and victim of abuse.
__________________
4 comments:
I just found you blog, and I feel like I've "come home" so to speak. We are dealing with a particularly tough time right now with our son, almost 7, who was adopted out of foster care at almost 5 years old. We knew we (and he) had hit rock bottom when we had to call 911 to intervene in a rage. Broke our hearts to do it, but we had to stop the violence before we or he were seriously injured.
So far, his dx is PTSD, attachment "issues", ADHD, anxiety, learning disabilities, sensory "issues" and depression. We now highly suspect early onset bipolar as well, and possible FAE. We are still on a very difficult journey to unravel his past to get proper treatment. It's been a very rough road lately.
Thank you for your blog. I'm feeling a little less alone today...
Take care,
Dawn
I just found your blog! We're in the midst of doing initial overnight visits with a 15 year old that we want to adopt out of the foster system. Sometimes I think we must be crazy - there is so little writing about this kind of situation. Thank you for putting your experience out there!
Hi Mary!
I'm so glad you found Heather's book helpful. The following books she published are even more in depth and adds more understanding, and her online classes (http://www.beyondconsequencesonline.com) based on the books really helped me to change my thinking for good so that I always know how to behave in the moments of chaos.
We adopted our daughter at age 10. She has been with us 3 1/2 years. It actually seems to be getting better for the most part - although the teenage years do scare me a bit.
She was severely abused, sexually, emotionally, physically, etc. She and her siblings often went without food as well. So you can imagine the issues she has.
With all that in mind, I believe the hardest thing for her is having to be separated from her siblings. She was in foster homes/childrens home since 6 years of age. She is the 2nd oldest child and was mostlikely the caregiver for the younger siblings.
She was mainly diagnosed with ADHD and ODD. From the start, I did not think she had ADHD, but thought her hyperactivity was more a symptom of what was going on in her brain. We have since been able to remove that label with the help of psychiatrist. What we did discover was that she was constantly nervous/anxious - no wonder with that past. Then I read up on RAD and the psychiatrist confirmed anxiety and put her on an SSRI: Zoloft. It has been a life savor for her and us. She is still somewhat anxious, but it is now managable.
She has since then been able to focus in school and not be labeled as difficult. Thank goodness, she is now in a school for children with special needs where she gets the attention she needs and is taught life skills. I'm not concerned whether she goes to college, etc. I just want her to become an indepentent and trustworthy young lady.
Blessings,
Barbaraturdine
Post a Comment